

Two years ago, I wrote a piece on social construction within the brain injury rehab context. The Executive Director of the Brain Injury Society of Toronto (BIST) on behalf of the Board approached me afterward in response. They were concerned that I didn’t feel safe enough to bring this issue up directly with them, and they wanted to create an Advocacy Committee and invited me to be the first member on it.
Tuesday night, January 26, 2021, I decided to quit.

The Advocacy Committee had its first meeting in December 2020, but due to a conflict between me and the Original Chair, the first meeting was reset. (Original Chair refers to first one designated as Chair before a Co-Chair was appointed.) The reset had a technical snafu; the reset of the reset aka third meeting occurred the week of January 25, after which I quit. I’ve thought about how much to write about it so as to not identify any one person yet highlight the problems. I hope I’ve succeeded. I think it’s important there’s an emotional landscape to my post, for humans think better and are more motivated to effect change when emotions are engaged. Having not volunteered at BIST before, I knew nothing about the functioning of its committees, and so I come at this from both the perspective of a newbie to the committee process in brain injury organizations and of a battle-weary self-advocate.
I want to preface by saying I like all the staff. I look forward to seeing them at the Community Meetings, and I think they work very hard for the members for little compensation. The Chairs of the Board, whoever they are and have been, have always had my back as have various members. And so I don’t write this post lightly. But I’m hoping, maybe, perhaps, it will result in good things.
Although I had wanted to quit months ago, feeling rather side-swiped by the delays and by the Original Chair conflicting with me long before the rest of the committee members were chosen, I hung on to the promise of it through two years. As presented to me, the idea was the Committee would discuss and decide on advocacy needs that they’d then present to the Board, and the Board would decide which to act on. In other words, the Board assigned the purpose or mandate of advocacy to the Committee, and the Committee would determine the specifics.
Mandate
A year ago, I learned that the mandate was determined not by the Committee but by . . . I’m actually not sure who. I know the Original Chair began setting a new mandate. They wanted to do a survey. I objected strenuously, for I had begun agitating for BIST to engage in advocacy after they had done a survey. Doing a new survey would be repeating something already done. In addition, asking committee members not trained in survey taking meant the results would contain their biases. Far better to ask Statistics Canada to do it, especially if the original survey was insufficient. Conflict arose and expanded into other issues between me and the Original Chair. The Board solved it by appointing a Co-Chair. However, they didn’t discuss it with me personally nor engage in conflict resolution. I figured the pandemic had thrown a wrench into a lot of normal things like that.
“The Board of Directors shall specify at least the following: [the committee’s] function or purpose; its limitations; its composition; and when and how often it shall meet. . . .Minutes shall be kept of all Committee meetings.”
The Original Chair didn’t appoint anyone to take Minutes at the first meeting, took them themself without us knowing at the time, and I pointed out errors in the emailed Minutes that exacerbated the conflict between us. This was partly addressed by not having the Original Chair run the next meetings. However, my self-advocacy didn’t result in conflict resolution.
By Fall 2020, the mandate had changed to self-advocacy. Well, speaking as a person who’s been self-advocating for 20 years fairly successfully and hasn’t recovered from the nightmare self-advocacy with brain injury throws you into, I very much doubt that’s going to change how badly brain injury is treated right now. The problem is too massive for individuals working alone. And I feel for anyone trying on their own with an injured brain to get what they really want: their life restored. No matter how skilled they are, they’ll be facing immovable, massive resistance to providing good medical care and inclusive city and public transit. It’s soul destroying.

Self-Advocacy
Has my self-advocacy one-on-one or through blogs, books, innumerable social media posts changed medical care for the majority of people with brain injury? No. Has it returned cognitive accessibility to the TTC? No. Did it get BIST to listen to my outrage over them doing nothing about racism? No. Did it get conflict resolution last year or this week with the Original Chair? No. The problem with self-advocacy isn’t that a person can’t do it, it’s that the receiving party isn’t listening. It is hard to hear what you don’t want to hear, tis true.
The worst problem is that self-advocacy for brain injury care contributed significantly to creating PTSD in me, and I’m sure that’s true for others. I wouldn’t wish that on my worst enemy. The only way to make people, governments, health care professionals etc. listen is for an organization to speak up. Groups can create solutions and brainwrite ideas that an individual cannot do on their own. The group has power the individual does not.
Yet over the years BIST has seemed loathe to use the power of their group in favour of supporting me (and I’m sure others) in our individual advocacy efforts despite all of us knowing those efforts would probably go nowhere. And so two years ago, I felt hope.
Agitating for Advocacy
I’d raised the issue of advocacy years ago because I’d become disillusioned after one particularly ineffective June brain injury awareness month when I wondered why BIST did not take advantage of free TTC advertising for the month to inform the travelling public what it’s like to travel the TTC with a brain injury: the cognitive challenges, the visual dangers, TTC’s attitude of non-inclusivity. It seemed to me that BIST was more concerned about the TTC’s feelings than they were about highlighting the challenges the disabled population face every time we board a bus, streetcar, or subway — or even visit the website to figure out routes and schedules. Yet one of the Board members had driven me to the 2015 TTC Access Meeting because they supported my personal advocacy for accessibility on the TTC. A staff member had notified me of and accompanied me to a meeting at the TTC with disability stakeholders after my eye surgery. And the Executive Director invited me to accompany them to speak to the CNIB, which apparently was well received. (Although it went well, similar visits to other organizations representing various disabilities did not occur with me for reasons unknown.)
Objective 2.5: “To advocate for social change in Toronto that will enhance opportunities for and remove barriers to participation for people living with the effects of ABI. . . .2.7 To encourage volunteers to become involved with attaining the above goals.” Volunteers can do that in a culture free of oppressive ableism and racism.
BIST did advocate in a sense for those of us forced to use the TTC: they fought successfully to get cognitive disabilities included for Wheel-Trans eligibility. The problem with that is that many of us don’t want to use the unreliable, privacy-breaking Wheel-Trans. I’m sure I’m not the only one not enamoured with giving my entire health information to the TTC, an entity that cards people with disabilities and, I assume, racialized people, too. (There’s been much talk about carding by police, but not by public transit as far as I know.) The TTC doesn’t need my medical records to know how to transit me safely. But the kind of paternalism evident in the way BIST advocated — by deciding to pursue Wheel-Trans instead of publicly and persistently confronting the TTC about their cognitive inaccessibility — and the kind of paternalism evident in the TTC’s 16-page intake form for Wheel-Trans, is why advocacy that listens to and respects those of us with brain injury and our variety of needs is so needed. To that end, recently, BIST launched an ABI Justice site for those caught up in the criminal justice system due to their (untreated) brain injury.
But we’re in the middle of a medical crisis of epidemic proportions, which the pandemic has massively worsened. First and foremost, we need advocacy to educate health care professionals to actually diagnose and treat people with brain injury appropriately and effectively. Standard medical care right now does neither. Through pinpointing damage and directly healing injury, you lessen all other problems that flow out of untreated and ignored brain injury: homelessness, criminal justice issues, bankruptcy, isolation, and higher risk of dementia.
“To Empower the Community to Advocate for Themselves: Through the dissemination of resources and/or strategies . . .”
In September 2020, I was told the Advocacy Committee was ready to launch with the self-advocacy mandate. In December, at the first meeting, the mandate seemed to have been narrowed down to one action chosen by the Original Chair: signing a petition. While the Original Chair talked collaboration, there was no evidence of it through this top-down approach.
Leadership and Meeting Styles
My other issue with that first meeting was the presumption as I understood it that the person most competent to chair a committee was a Board member. I disagreed with the idea that only a Board member could chair a new committee. A little background on me:
I belong to a fraternity. My fraternity trains all of us extensively in how to run meetings and events efficiently and with the ideals of sisterhood empowering us all. I’ve run meetings and organized a regional meet encompassing New York and Ontario. I know I’m not the only non-Board member who has a background in meetings and business. That’s why I felt the Board’s assumption about who should chair a committee was based more on status conferred from Board membership than actual competence and experiential background.
And so I expected some social chit-chat before the meeting was brought to order and then it to be run according to Roberts Rules of Order. Instead, whereas my fraternity gives meeting dates weeks ahead of time along with agendas, we were given little notice. Whereas my fraternity provides the agenda weeks ahead plus any necessary documents, we received the agenda only 24 hours prior and only after I prodded the Original Chair for it, and we received no documents. Whereas my fraternity designates a person to take the minutes, this did not happen at the first, second, or third meetings. Whereas my fraternity includes all voices in decisions and resolves conflicts, the meetings weren’t run to encourage all voices and a needless very serious conflict arose in December that lead directly to me quitting.
In addition, I believe I wasn’t the only one stunned to see legal documents for the first time when screen shared during the meeting.
People with brain injury need time to read documents, including one-page agendas. We have varying levels of fatigue, slow processing, and difficulty reading. Assuming 24 hours is sufficient time or presenting for the first time at the meeting reflects either ignorance of how brain injury manifests or a flippant disregard for the need for processing time or incompetent prep. Besides, it’s just considerate. I learnt that the Original Chair didn’t work on the agenda until the last minute. Brain injury interferes with good time management and kiboshes organizational skills, but if the Original Chair has issues with that, why were they made Chair when members exist who wouldn’t have those issues or would know how to compensate for them?
Codes of Conduct
Worse than the last-minute agenda were the mandate and code of conduct, which from their file names were written in October yet not emailed to us back then to give us plenty of time to read, process, and respond. Also, I simply cannot comprehend why anyone would think that people with brain injury can read such documents, why they were not kept to one page, and why plain legal language wasn’t used. I only received the code of conduct in my inbox this week.
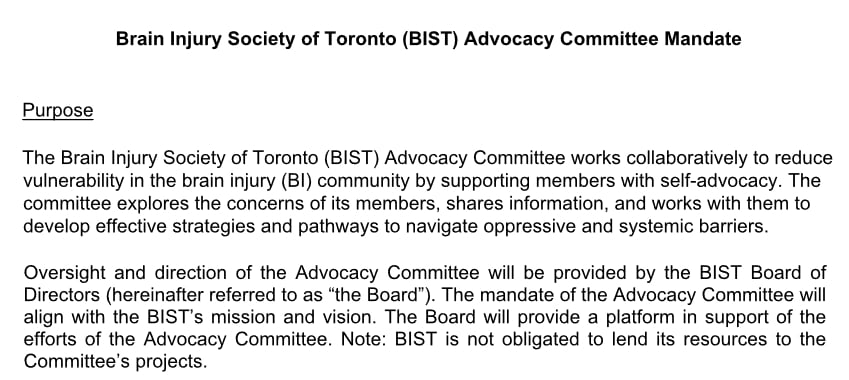
The Code of Conduct for the Advocacy Committee begins with “Expectations and enforcement of the ground rules for the Advocacy Committee fall in line with the BIST code of conduct.” Then followed a lengthy legalistic document. I wondered where to begin with the condescending document? Maybe look at what the writer supposedly based it on?
The BIST code of conduct for members is really negative, as in adjuring, lots of finger-wagging “nots,” the sort of thing as a person with brain injury you hear a lot. Bad behaviour even in brain injury community is not common. This sort of document creates an atmosphere of mistrust, oppression, and patriarchy, the opposite of comfortable when you have to second-guess your behaviour the moment you enter BIST domain. And that’s speaking as a person who stirs things up but doesn’t wear offensive clothing, manages to mostly keep her language clean, doesn’t touch people, turns off her phone, videos only speakers and after asking, etc., but whose cultural and brain-injured way of communicating are not within the white North American norm. Not even children are subjected to this assumption of needing to be disciplined before even showing up anymore. Just because something has become standard fare doesn’t mean it’s good. Look at standard medical care of brain injury.
People who have no affect from their brain injury could potentially manage the white male utopia of emotionless communication as laid out in the Advocacy Code of Conduct (which I just learnt will be reviewed) or people who are mostly silent could manage the artificially constructed concept of perfect communication, but not those with injury to their frontal lobes that affect emotional control or injury to temporal lobes that involve language. Then there’s injury to ability to literally think. Are they to be disallowed on the basis of the site of their injury? How is that equity? What about those who cannot speak without being given permission? Or those from cultures that express themselves passionately and vigorously? Furthermore, women are characterized by men and women as aggressive when they’re being as assertive as men.
During the December meeting I managed to spot one serious issue in these documents: the potential for silencing my writing. Apparently, others felt the censorship, too. Upon perusing the document again this week, I spotted other issues that I first encountered several years ago.
“Posting opinions . . . on social media forums, website(s) or blog(s), or other public forums that could potentially harm the reputation of BIST, its stakeholders or members, the Board, or the Committee.” Although this has now been conveyed to me that it’s a draft, this is not the first time I’ve encountered something similar. The word “potential” can be interpreted in the eye of the beholder not in actuality. So in other words, this post could be nixed. I’m a writer. I write to process, to understand, to remember, to calm my nervous system down, to express myself. Writing is breathing.
The BIST zeitgeist when I joined in 2009 was easy acceptance of people talking, interrupting, being their full glorious brain injury selves. I felt freed to be me, and thus reach my full potential functionality during those meetings. A few years ago, that culture devolved into a parental model of treating us like children with behavioural issues and enforcing a judgemental, unrealistic code of conduct upon us, a code of conduct that’s less about respect than it is about trying to force people with neurophysiological damage into some white male or health care professional’s concept of good behaviour. The racism I sensed in BIST, I see in full view in this code of conduct, a perception confirmed by a zero tolerance policy that was included in the Advocacy Committee draft.
Personally, I think we’ve seen from the school system that zero tolerance is an ineffective relic of the Premier Mike Harris era and has no business being in a document that governs people with brain injury who face judgement, paternalism, and complete misunderstanding of their neurophysiological deficits daily. Despite the fact that I wish to never see two particular people again, who in my perception abused their power imbalance and tag teamed me, I don’t believe zero tolerance is in order.
Conflicts Need To Be Resolved
During the escalating conflict, the tag team tried to silence me, informing me that meetings are run by having each person speak for a set amount of time, for example, five minutes. I was informed this is how professionals do it. And if I wanted to speak for longer, I needed to ask if another would donate their time to me. I’ve never heard of a more authoritarian, anti-brain injury method that’s guaranteed to stifle creative thinking, idea generation, and conflict resolution. People with brain injury have communication issues. Sometimes, you can’t speak for all the chocolate in the world; sometimes, the mouth runs off at full steam; and sometimes, you don’t know what it is you want to say and you have to keep going until you finally hear it coming out of your mouth. When it happens to others, I go along for the ride because that used to be the BIST way. It’s easy to interrupt a person with brain injury, the only potential problem being that you can stop them finding their way to the point they want to make.
Imposing a time limit ignores reality while creating stress that would hamper expression. Dumber than two fucks. Oh yeah, apparently we’re not to swear. How is it they don’t know swearing is resistant to injury and that’s why many use it to compensate for missing vocabulary? Are we supposed to say to those who can’t access their vocabulary but can access swear words, that they cannot speak? The dress code is offensive because it’s couched in negative terms that’s aimed at those with brain injury whose perceptual abilities and learning styles are sufficiently impaired that they may not understand that a porn picture on a T-shirt (assuming that’s what BIST means) is not on. And yeah, misogynists exist everywhere. I can see members spotting such a T-shirt, bluntly telling the wearer to take it off or leave because bluntness is a communication style after brain injury. Far better to present this sort of thing in a positive way. And no, I’m not going to tell health care professionals how to do that. It’s past time they used their little grey cells, that the disciplinary method left the yard and was replaced with creative, uplifting ways. In all my decades of fraternity meetings, using a stopwatch method, policing language, and imposing a dress code didn’t come up. We use human means to ensure equity and respect in contributions. We treat each other as adults of good will.
Good leadership, effective meetings, and employing brainwriting ensures respect, collaboration, and equity in all voices being heard without censorship, silencing anyone, paternalism, and oppression.
Changing Mandates
Meanwhile, the mandate has changed again. We heard that the new mandate was to be communication. Whoa! I totally understand the need for communication, but communication is not advocacy. Clearly, BIST is seriously bad at communication. It cannot seem to acknowledge the seriousness of a conflict, understand it requires conflict resolution, resolve issues in a way based in reality not on some social construct of conduct codes and “ground rules,” and reach out to people like me who are functional adults but are treated like children needing disciplinary daycare. These issues aren’t restricted to BIST. They seem to be endemic in the brain injury sphere. But the solution is not to coopt the Advocacy Committee but to create a Communication Committee or, you know, start listening to the members and stop being so paternalistic, judgemental, systemically racist, and lacking knowledge that brain injury effects are neurophysiological not behavioural in origin. If BIST feels it has a communication issue, in not being able to reach some segments of the population, perhaps they need to self-reflect on their inability to listen. If you listen but don’t act to change, then you’re not listening.
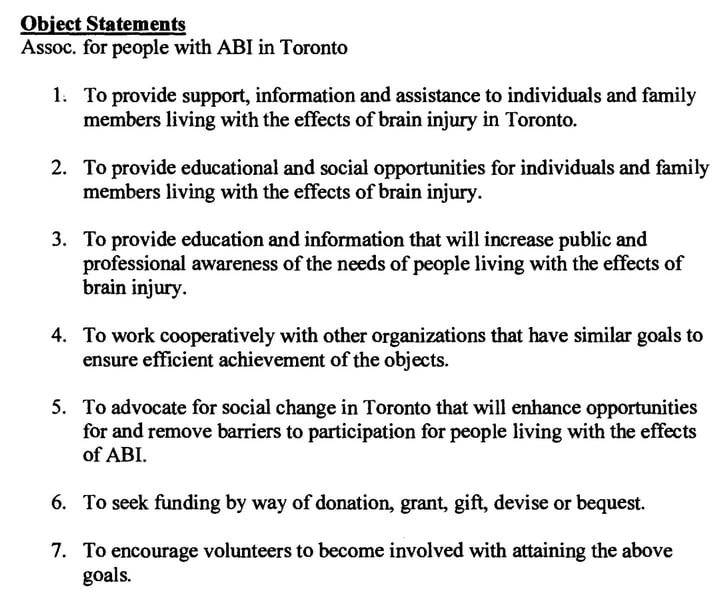
By the summer, I’d become impatient. I submitted a request to the Charities Directorate for BIST’s public documents several months ago and received them days before the third meeting. I reviewed the documents and noted that the original seven object statements when establishing BIST included:
“3. To provide education and information that will increase public and professional awareness of the needs of people living with the effects of brain injury. . . .
5. To advocate for social change in Toronto that will enhance opportunities for and remove barriers to participation for people living with the effects of ABI.”
BIST’s mission statement as it currently appears on their website:
“Our mission is to enhance the quality of life for people in the City of Toronto, living with the effects of acquired brain injury through education, awareness, support and advocacy.”
Dreaming Big
Social change is ambitious, a motivating and exciting thing, rather along the lines of what I’d like to see. As I see the approaching tsunami of COVID-19 causing thousands and thousands, perhaps multiples more, to have brain injury, I feel the urgency of transforming our medical system to properly understand, diagnose, and treat so as to restore people to their lives, even if not fully, at least significantly so that they don’t end up alone and friendless, or on the streets, or in despair permanently. The solution to homelessness, people ending up in the criminal justice system, and other terrible consequences is to actually heal the injury like doctors do cancer or broken bones. We need real advocacy that foundationally changes lives. That’s why I’m developing a brain injury site that encompasses education, diagnosis, treatments, support, how to choose a treatment provider, and looking to the future. I’ve been mulling it over in my mind for years as an extension of my book Concussion Is Brain Injury: Treating the Neurons and Me. The pandemic gave me the opportunity to start for three reasons:
- I no longer had my energy vacuumed up by the TTC.
- I no longer could attend medical appointments and had energy freed up from that to devote to other things.
- Back in the spring, I gave up on the Advocacy Committee convening any time soon.
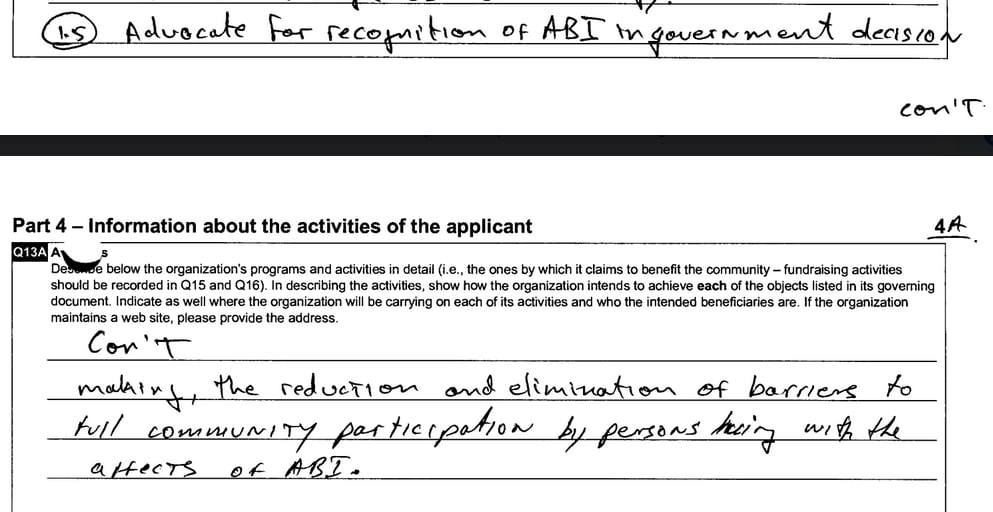
“Advocate for recognition of ABI in government decision making, the reduction and elimination of barriers to full community participation by persons living with the affects (sic) of ABI.”
BIST used to dream big. That paragraph is inspiring!
BIST can still dream big and radically alter the course of people’s lives into hope and full participation in Canadian society.
How could the Advocacy Committee have reflected the original aspirations?
What I’d like to have seen is the Committee collaborating on determining the mandate. While the Board determines it’s advocacy, broadly speaking, the Committee narrows down what is the most important and would have the most meaningful impact.
A mandate to effect social change requires thinking big. Thinking small as in petitions and self-advocacy leads to PTSD in people with brain injury. Thinking big is what leads to incremental change and, if we’re lucky, a giant leap forward. We with brain injury have limited energy. Put those energies to what is the most important and what provides the most meaningful impact. Right now, that’s educating the medical profession.
That’s what my experience and knowledge show me.
Yet I’m one voice. The best way to determine the Advocacy Committee’s mandate and its initial priorities would be to use creative thinking.
Brainwriting
Brainwriting is a creative thinking method that harnesses the power of the group while putting every voice and idea on an equal footing. Brainwriting provides a way to sift through ideas in order to develop a good one or two. You need a collaborative virtual platform to do that, not the racist and marginalizing Zoom. If BIST wants to shed itself of systemic racism then it needs to look at the technology it uses as well as the language and assumptions in its documents. Choosing comfort over the right thing to do by choosing to stick with Zoom, for example, basically allies with a technology whose free offering is based on the idea that marginalized are inherently criminal and whose interface is cognitively confusing.
Learning a new virtual platform is hard. But people of good will support those who are anxious about the learning curve, leading them to increase their sense of competence. This is a good thing. (And, after all, everyone had a learning curve with Zoom.)
Using a collaborative platform, you can employ a brainwriting technique like 6-3-5. You could modify it to have everyone take 5 minutes to write down three ideas related to advocacy. I think those who assert I talk too much is because they want to maintain the status quo and I’m assertive and passionate about not doing so. They don’t see that others’ silence isn’t because a couple of us speak a lot; it’s because some, like I often do, are using all their brain resources to process; some are shy; some are simply observing. That’s why brainwriting was developed. It’s a way for the shy and those who have a hard time processing and responding in real time to have equal say.
I’d write down educating medical professionals.
We’re in a crisis and the numbers of disabled will swell beyond our society and BIST’s ability to support if they are not provided with diagnostics and neurostimulation therapies that heal brain injury so that they can return to work, play, and their social networks.
If educating health care professionals was the consensus, then the next round of creative thinking would be on how to do that.
Once the Committee has made a decision, we’d divvy up the responsibilities and go to work. One year is not much time to get anything done, especially for an organization that took two fucking years to launch a committee. And, as well, the Committee will need time to set up its approach to advocacy, how it’ll operate, how it’ll mine the skills and time of BIST members, and so on. But at the end of the year, as part of the Annual General Meeting, we could present a review of what was accomplished, what was left to do, and how to build on it. That’s motivating and purpose driven!
People with brain injury represent the population. Some are very wealthy. Some live on the streets. Some are chronically ill. Some are able to work full time (albeit with lots of support, I’m sure). Some live alone. Some live in extended families. Some are rejected by their family and friends. Some live surrounded by support. What we all have in common is that we’re adults. We want to live and work and play with self-determination. We want to have our brains back.
I can see so much possibility in what BIST could do to effect that. But the desire doesn’t seem to be there. So I’m moving on. I have better things to do with my limited energy. And this has sucked up too much of it already. Perhaps a person with infinite patience and endless optimism can reverse BIST’s devolution to top-down paternalism back to its treating adults like adults and aiming for social change. I know such people exist, for I see them in politics and am impressed with their boundless optimism that some day real change like universal basic income will happen. Perhaps my strength is in agitating from the keyboard and sharing my knowledge through books and websites. I know I’m good in groups, just not those with people who like to control others and exert top-down oppressive patriarchy.
