
I wrote last time about my reading evaluation. This post is on my results. When you have a brain injury and rehab tells you that you can’t read anymore, you assume that they’ve done a thorough assessment and analysis of your reading cognition.
You’d assume wrong.

Reaction
In 2005, five years after I was told I wasn’t reading the ubiquitous mass paperback in my hand, I had a qEEG done, which told me the neurophysiological basis for why I had so much difficulty reading. The first week of June 2018, I underwent three hours of testing over two days that assessed my auditory, visual, and language foundations of reading; my fluency; my comprehension; and my concept imagery.
Huh? Yeah, I’m still learning these too. They match with my experience, but they introduce concepts that I haven’t heard of before or only knew about from a different perspective. I learnt more about where my reading difficulties lie.
My very first thought was: why did I not have these tests done during rehab in 2000? Why did the medical system not assess all my cognitions with full, appropriate qEEGs and these kinds of reading, writing, and math tests?
If I had been properly assessed, not just given a neuropsychological test people with high intelligence can ace, injury or no injury, I would have had a complete picture and been given a precise scientific and medical explanation of why I couldn’t read anymore, not just a general statement of you can’t read.
I also don’t even know how to process the fact that when I asked my neuropsychiatrist for help with reading that the reading expert he consulted pointed to the aphasia website and didn’t tell him that I should have all these tests done, the ones I’ve just undergone. It’s been bad enough I had to wait twelve years for a reading “expert” advice, but to have not known about these tests for a further six years because the medical and “reading research” community are so intellectually lazy is beyond egregious. I’m pissed. And upset. And filled with hope that finally I’ll get my book time back.

I’m still processing my results.
Results
It’s difficult to explain what one is only just starting to grasp. Lindamood-Bell who conducted the evaluation, normed all results to my age and gender.
- My reading rate is too slow. I’m in the 16th percentile. That means 84 percent of women my age read faster than me. I believe this rate is about double what it was in 2001. Wow! Some progress!! sarcasm
- My foundations are solid. These are the ability to hear phonemes, the sound parts that make up words. The ability to recognize and pronounce high-frequency words. The ability to figure out an unknown word within the context of known words.
- I rely on my vast knowledge bank and familiarity with language to prop up my comprehension. When I cannot see a word but only hear it and I have to pick out an illustration that best represents the word, I cannot rely on my ability to decode a word from its roots to figure out what it means. And so I don’t do so well. Based on results from standard vocabulary tests, I drop about ten percentile points, maybe a bit more, when given the same vocabulary test when heard, not seen, and using pictures instead of words to “define” the word spoken to me.
- My accuracy in reading words is very high.
- Fluency is rate plus accuracy. So my fluency is not at the level that my reading foundations indicate it should be. (Slow reader.)
- When I can rely on my knowledge bank and ability to decode words, my comprehension is good. When I read new or lengthy material even text at grade six level, where I can’t rely on my knowledge of content and language, my comprehension drops a lot.
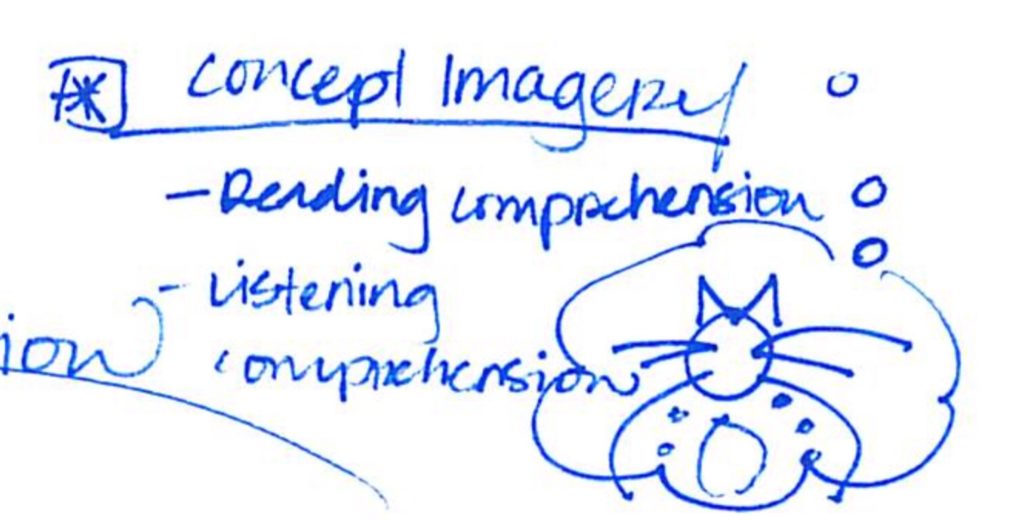
- Concept imagery is the ability to conceive a word, sentence, or idea as a whole in a kind of picture. I don’t have it. It’s sort of, uh, depressing . . . more than that . . . grievous and devastating to see one rated as having a mental age of 14.5 or 13.5 years in these tests after eighteen years of rehab, active treatments, and passive home treatments. On the other hand, they confirm I’m not imagining my reading problems. I have real difficulty despite the fact that I’m “articulate” and can read words no problem.
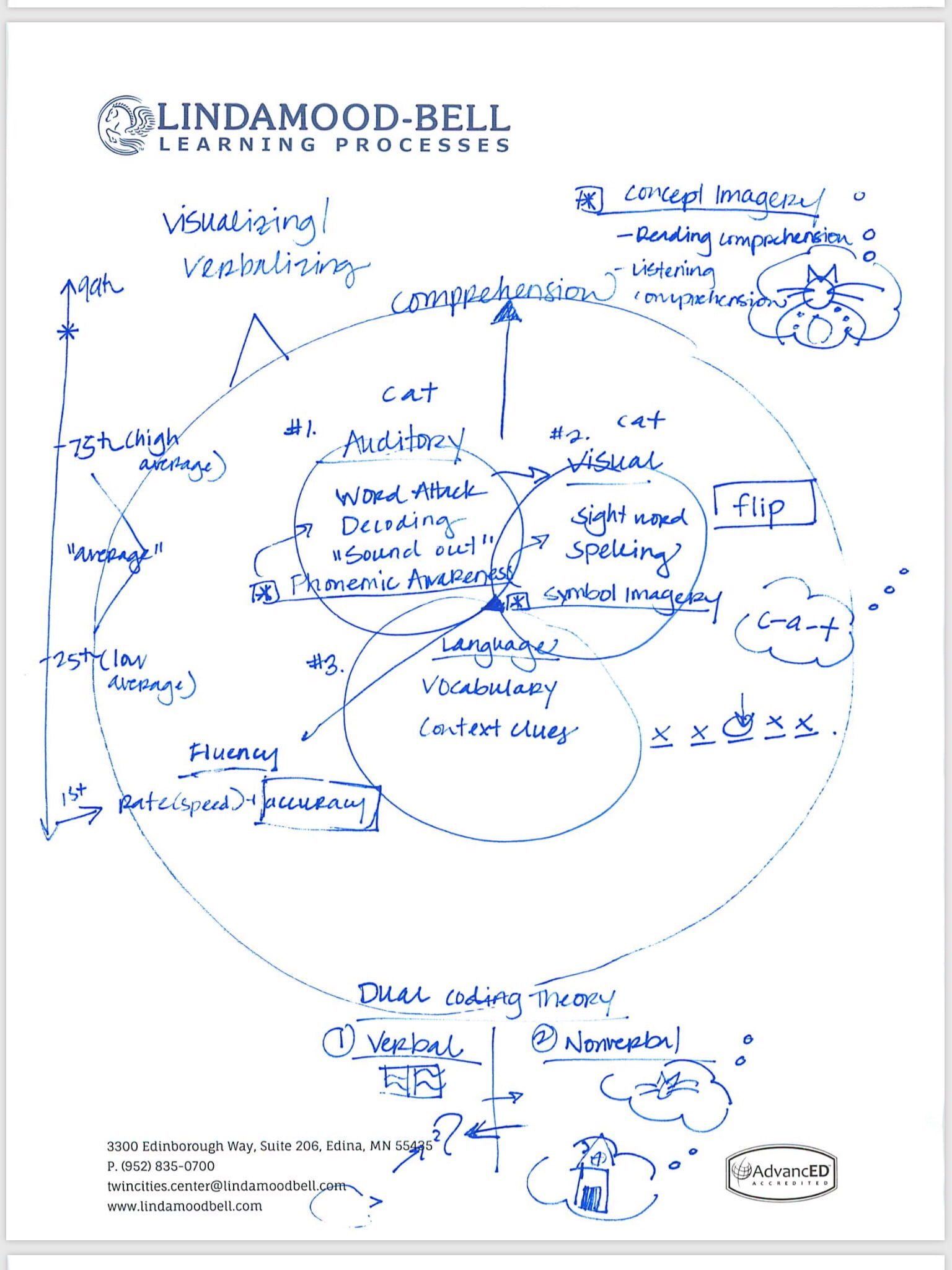
As I understand how Lindamood-Bell conceives of reading, reading comprises decoding and comprehension. Decoding is done in the reading foundations aspect of reading. There are three parts to reading foundation: auditory, visual, and language.
“. . . thinking that reading is decoding a word but reading is being able to comprehend.” Nanci Bell
Auditory
The ability to hear phonemes, the sound parts that make up words.
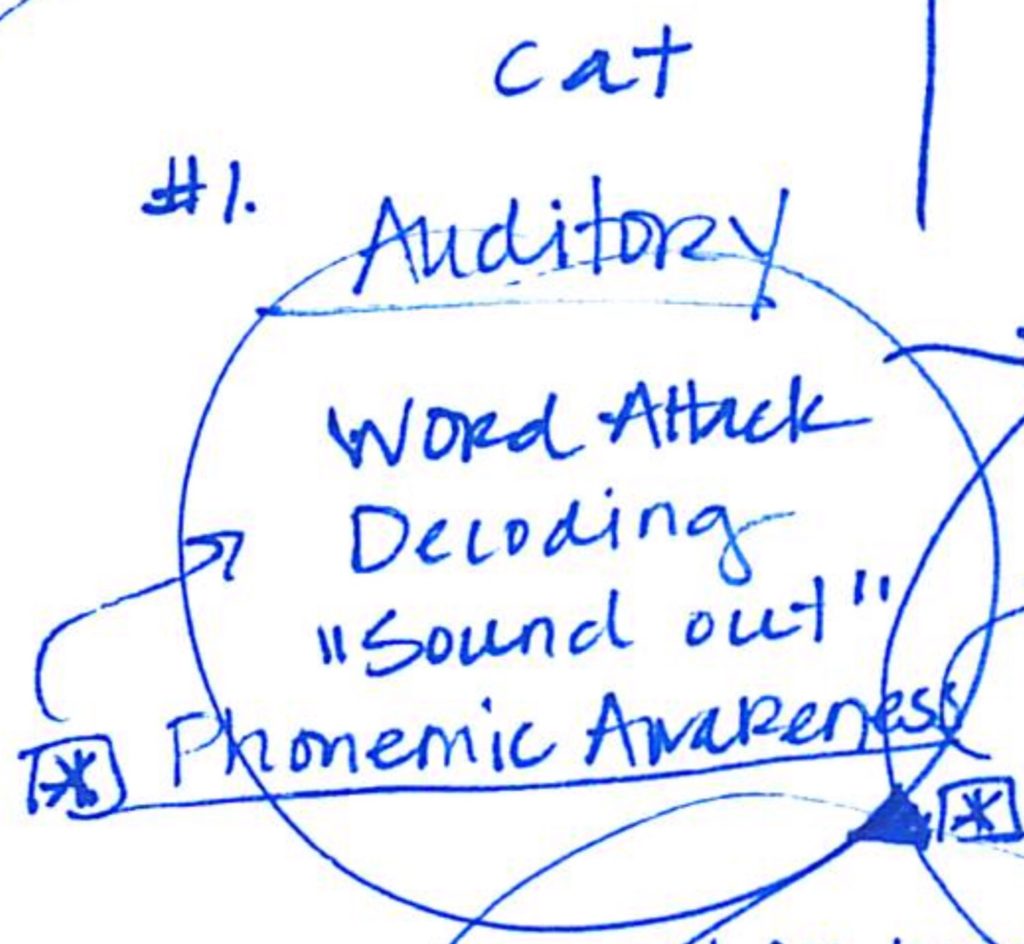
Visual
The ability to recognize and pronounce high-frequency words. The ability to spell high-frequency words, that is, words that are used often in everyday reading. And the ability to image symbols, that is, letters or letter combinations.
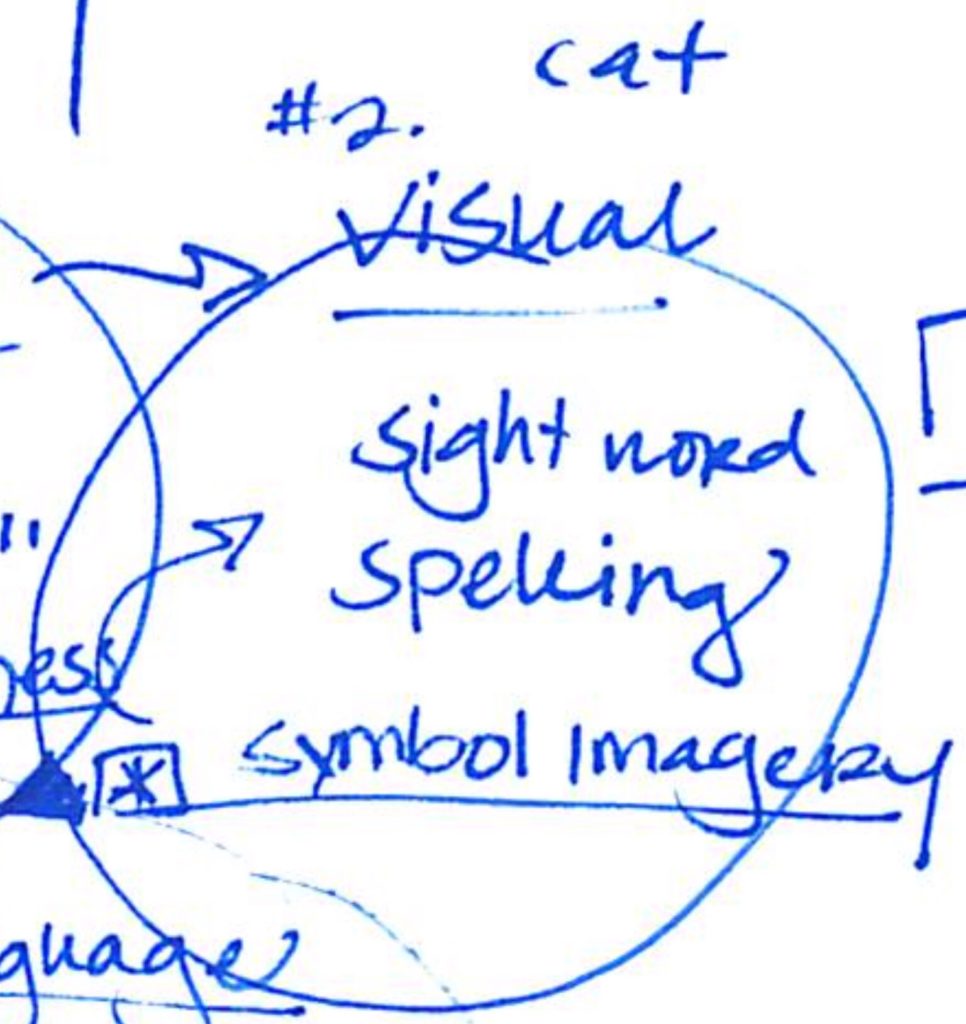
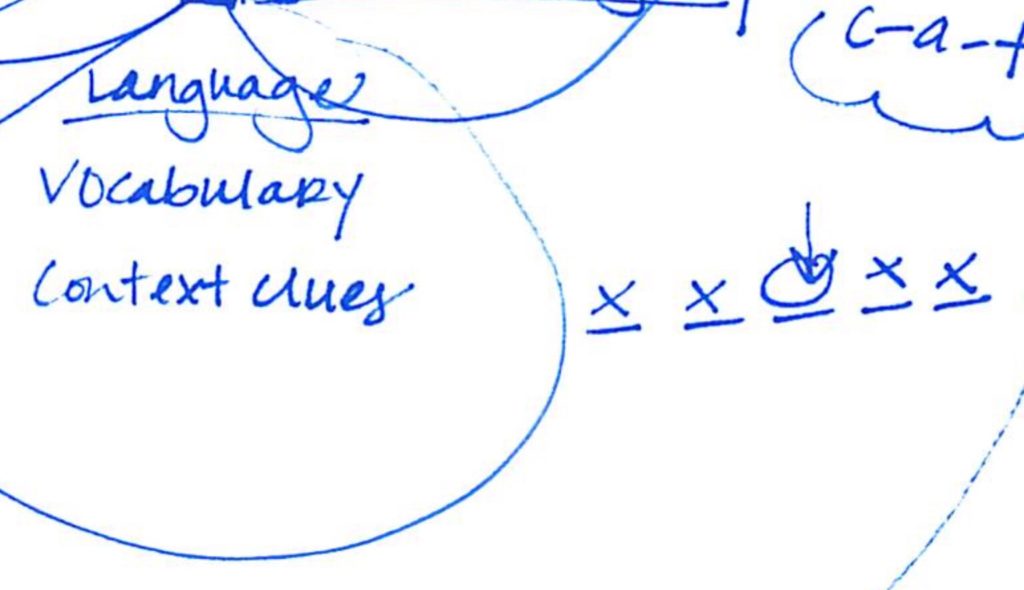
Language
Vocabulary. And the ability to figure out an unknown word within the context of known words.
Encompassing these three foundations of reading is comprehension.
“If there’s weak comprehension, … frequently teachers and parents don’t really know perhaps there’s weak comprehension. . . . If it’s really severe could be labelled hyperlexia there’s a gap between ability to read words and ability to comprehend. Or if it’s weak enough, it can fall into the label of autism.” Nanci Bell
Comprehension
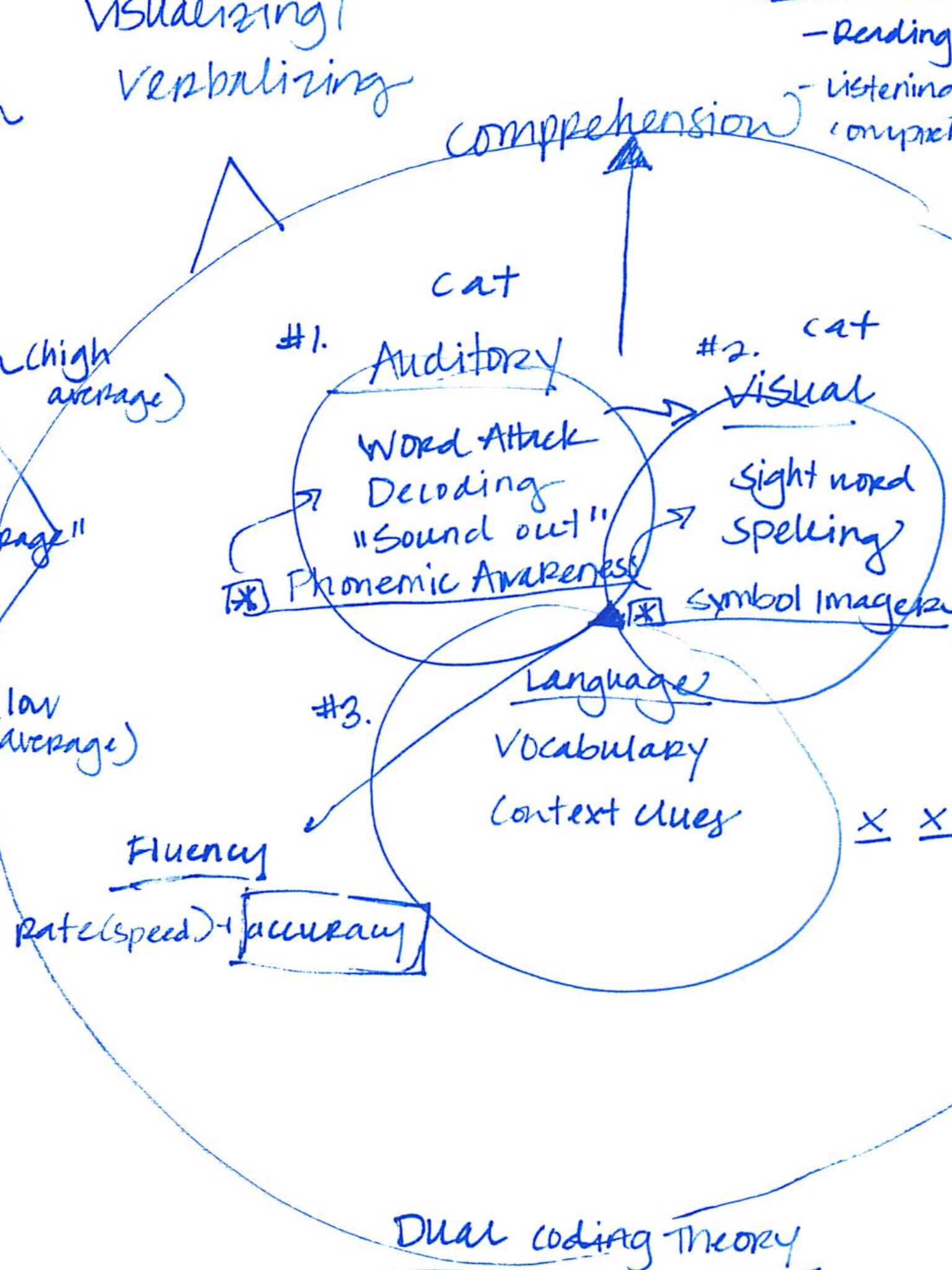
Lindamood-Bell uses Dual Coding Theory to explain how what we decode while reading — either text or listening to the words — is turned into comprehension by our brains. In dual coding theory, the symbols — words on text or words heard by the ears — the auditory, visual, and language parts of reading — are turned into non-verbal concepts that we can picture. A painting represents a thousand words and all. (Wikipedia notes it was a Canadian who posited this theory. Why is it then Americans, not the Canadian rehab centre I went to, that knows about and uses this theory to rehab reading?!!!!)
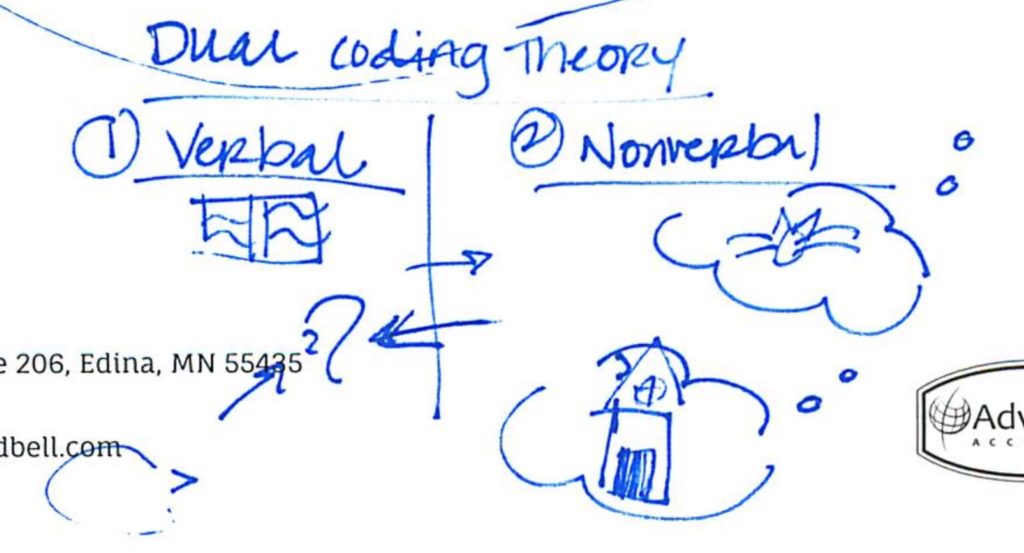
As part of that theory, they posit that concept imagery is how we understand what we’re reading. When we read or listen, we create a picture in our mind of what we’re seeing or hearing.
Nanci Bell, co-founder of Lindamood-Bell, explains the comprehension and concept imagery side of reading in this video below. Note that what we often think of as reading issues, eg, dyslexia, occurs on the decoding side of the ledger. The comprehension side isn’t usually talked about. It usually doesn’t even have labels like the decoding side does. I personally don’t think labels are always useful, but in our current milieu where everything is labelled, a label gives credibility. I think that’s why when people with brain injury say they have trouble reading yet can read words and use some or a lot of their vocabulary, health care providers, family, and friends don’t believe us. But as Bell says, vocabulary is not comprehension.
Now comes the tough part.
Restoring Book Reading
Lindamood-Bell said: “we can restore your book reading.”
Pause.
“What’s so tough about that, Shireen?” you might ask.
This is like where I describe in my book how I met clinicians in 2005 who knew what I wanted — to heal my brain — and said they would help me do that and could. It’s so hard to describe in a blog post what it’s like to be neglected medically, your angst and desires dismissed, and told to accept diminished functionality for years and years and then be told you can be helped significantly — and then you find out the help was available at the time of your injury; it’s just that the people entrusted with your care didn’t know about it or “believe” in it and your loved ones never searched for you.
Once again, I’m being told the unbelievable, that what I’ve wanted for years is in fact doable. It feels untrue. I asked:
“When you say I’ll be able to read a book like I used to (before my brain injury), do you mean a book at the level of an Agatha Christie? A PD James? Neuroscience article? And/or philosophy of mind textbook?”
They answered:
“In creating your recommendations for instruction, the goal I had in mind was your ability to read and process literature at the level of your potential, and at the level that would support research and continued learning for your writing. Especially with the full recommendation of 120 hours, I picture your ability to access all of the examples you provided in your original question. Our instruction may start at a lower level, but over the daily and weekly sessions, you’ll see an increase in the amount of language (text) you are processing as well as the complexity.”
Basically it would look like an ascending ladder of difficulty.
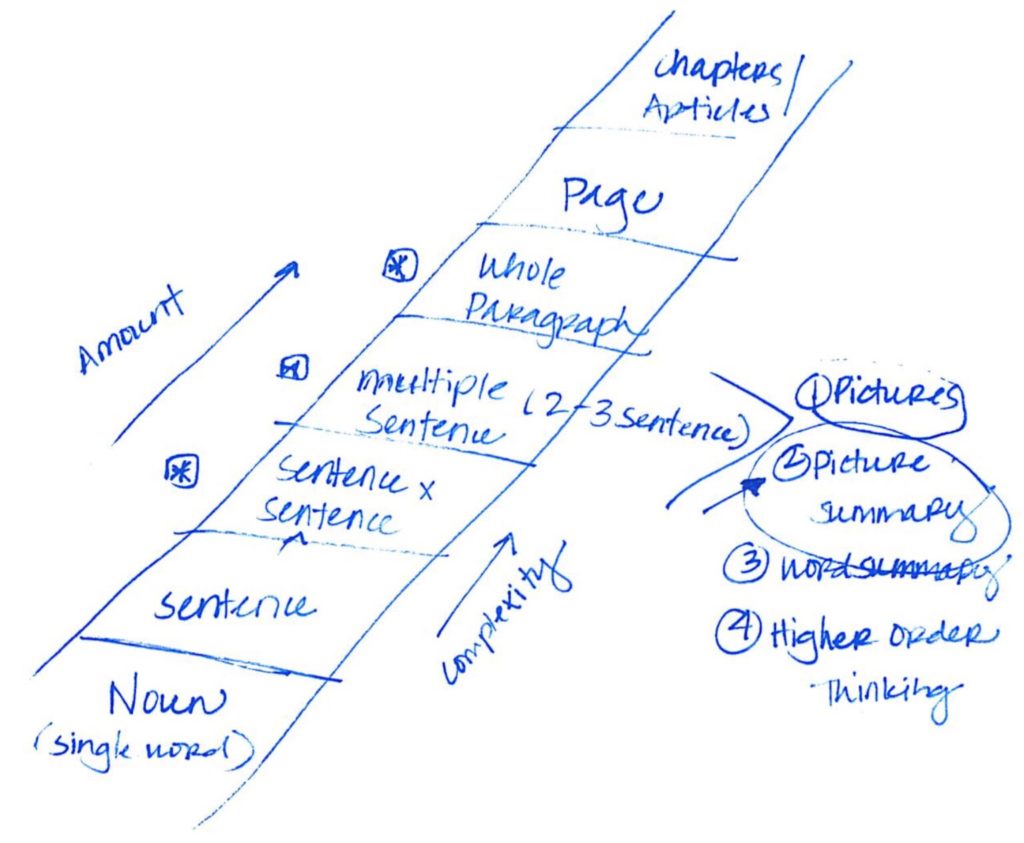
They continued: “Since our vision for instruction will include increasing the volume of information you are processing, our goal is to decrease your fatigue, by systematically and consistently reinforcing independence with visualization for increasing lengths of language. Just like any foundational skill (ex: learning a new language, learning a new instrument) practice and continuous exercising of the skill, makes it more automatic. Instruction will stimulate and strengthen this process for you, but practice outside of sessions and beyond instruction, will also be key. You may still need to take breaks, but I anticipate the length of breaks and the frequency of breaks will diminish as you, on a daily basis, start reteaching your brain this visualization process.”
I’ve consulted with some of my health care team. They believe I will benefit, that I need this hope. There is some skepticism that reading books like I used to is achievable; but no matter what, given all the brain work I’ve done, how my brain is now used to training, and how I do the work given me, I will benefit. My reading will improve. Dr. Lynda Thompson at the ADD Centre, who referred me for evaluation, was impressed with the time they gave me answering my questions and liked that they would show the objective learning curve not rely on subjective feelings and measure the gains.
I’m not sure how I’d be able to handle it if I didn’t achieve reading like I used to, though. That’s why I’ll need all the support I can get from my neurodoc. We’re patching things up; I’ve enforced pursuing my goals, and only my goals.
The normal intensity of instruction is four hours per day, Monday to Friday, for four to six weeks. Because of my fatigue, we’ll cut that down to two hours per day, five days a week, for eight to twelve weeks. It seems that I would need the whole three months and would have to practice daily on top of instruction as well as continue daily practice after instruction ends. Whew. That’s a heck of a commitment to work! I worried that the whole thing would be a moot point if I didn’t find a way to pay for it. I need help since the cost is way, way beyond my means. So I’m borrowing. What else is new.
OHIP really should be paying for this. This is what cognitive therapy ought to encompass when acquired brain injury clinics talk about what they do as cognitive therapy. It should also include brain biofeedback and audiovisual entrainment and long-term talk therapy. But first we need to get the medical system to assess cognitive functioning and brain injury properly. And to get anyone working with people with brain injury to take their reading problems seriously. We live in a knowledge economy after all — if we can’t read volumes of information, we can’t work.
Concept imagery underlies comprehension. Comprehension not based on having an adequate vocabulary nor ability to hear phonemes. Nanci Bell: “What they struggle with is the concept or the whole. And if you don’t have the whole, you can’t do higher order thinking skills such as main idea.” They call it in the U.K. aphantasia, the inability to visualize. Higher order thinking: From what you pictured— not what you think — what comes next in this story?
Lindamood-Bell trains to the client’s potential not what falls into the average range. This is significant. Brain injury rehab is about working to the average of what they’ve done since the 20th century, not for what is needed for independence, satisfying functionality, and most importantly, the person’s potential.
—–
Sketches courtesy of Dana Kernik-Theisen, Center Director, Lindamood-Bell Learning Processes, Edina, Minnesota, who generously gave of her time to explain my results, recommendations, and reading theories.
